Brain protective ventilation strategies in severe acute brain Injury
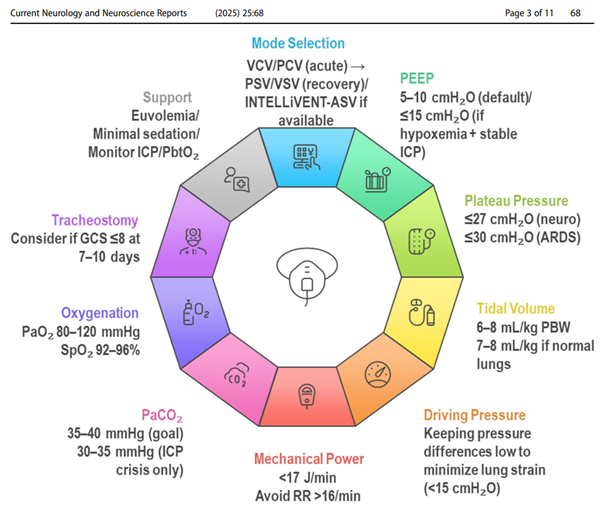
There is a need to individualize ventilator settings to preserve intracranial pressure (ICP) and cerebral perfusion pressure (CPP), while maintaining lung-protective strategies. Key recommendations include prioritizing physiological targets over ventilator modes, judicious use of positive end-expiratory pressure (PEEP) with concurrent cerebral monitoring, limiting plateau pressures, and maintaining tidal volumes within protective ranges. Minimizing driving pressure (ΔP) and mechanical power (MP) is emphasized to reduce the risk of ventilator-induced lung injury (VILI). The review underscores the importance of precise control of arterial carbon dioxide (PaCO₂) to regulate cerebral blood flow, avoidance of both hypoxemia and hyperoxia, and the integration of multimodal neuromonitoring to inform ventilatory decisions. Additional considerations include the potential benefits of early tracheostomy in patients requiring prolonged ventilation, as well as the influence of sedation depth, fluid management, and autoregulation monitoring on outcomes.
Thanks to the authors.