Surviving Sepsis Campaign : international guidelines for management of sepsis and septic shock 2026
The Surviving Sepsis Campaign (SSC) guidelines are intended to support clinicians caring for adult patients with sepsis, focusing on management in the hospital, the immediate prehospital setting, and the immediate post-hospital setting. These guidelines incorporate principles of antimicrobial stewardship through responsible antimicrobial use, proper diagnostic strategies, and deescalation of antimicrobial therapy. The recommendations reflect evidence-based best practice, distilling a large body of research into actionable recommendations. They empower individuals and health systems to make informed choices about care and support improvements in management and outcomes of sepsis.
Key points :
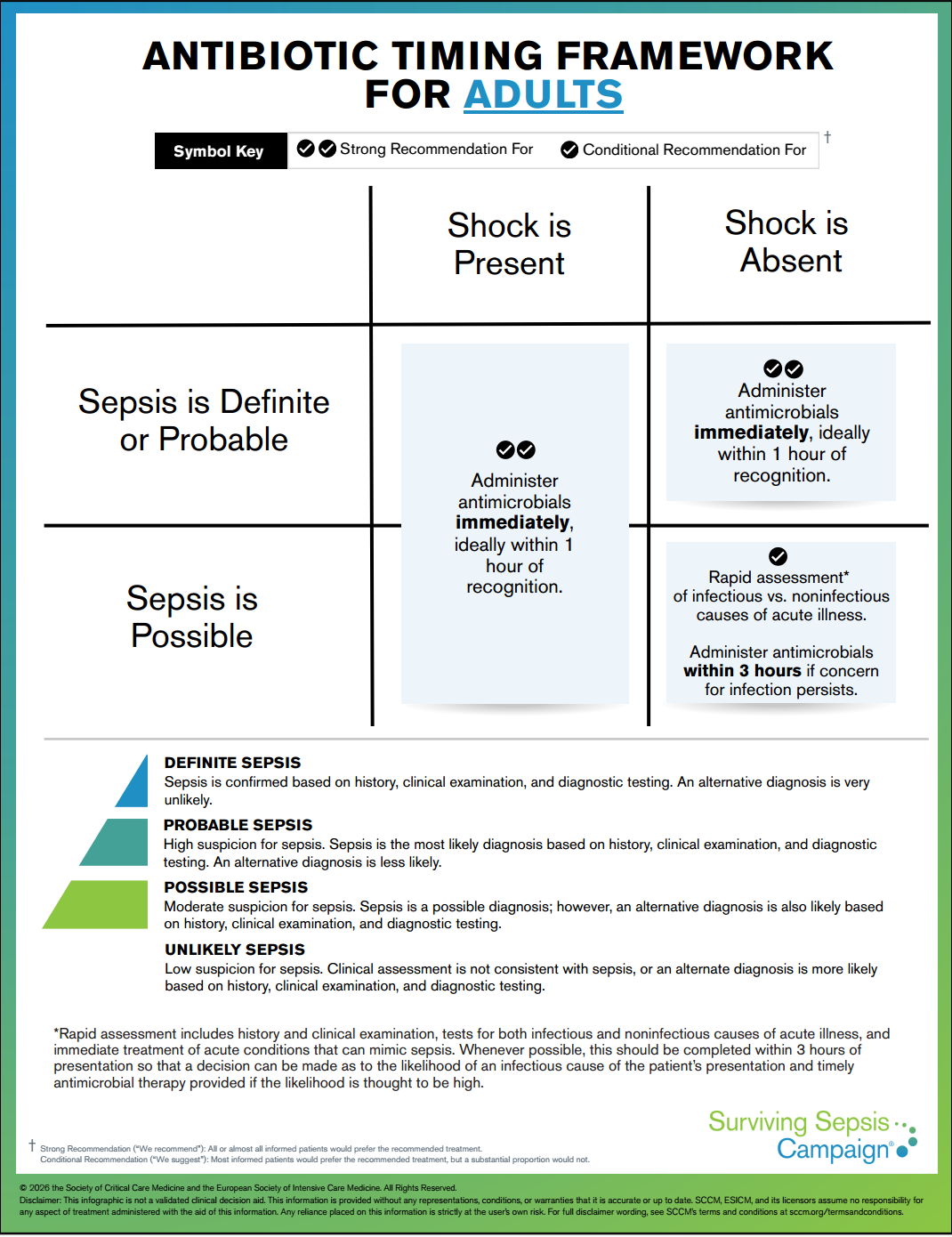
Early identifcation and treatment are critical to improving outcomes.
Sepsis = life-threatening acute organ dysfunction due to infection.
Septic shock = a subset of patients with circulatory dysfunction that confers a higher risk of mortality.
Quality improvement (QI) initiatives likely improve sepsis processes of care and may have small effects on mortality. They are recommended as part of a systems-based approach to improving sepsis management. Further, the integration of a performance improvement program for sepsis, including screening of high-risk patients and standardized treatment protocols, within existing antibiotic stewardship programs can enhance overall patient outcomes and optimize antimicrobial use.
The panel assessed that the balance of evidence favored the implementation of a multidisciplinary “code sepsis” response to improve outcomes in patients with sepsis (the benefit of implementing a code sepsis protocol likely varies across hospitals and health systems depending on the quality of usual care).
Four systematic reviews and meta-analyses have reported that Early Warning Scores (EWS) including NEWS, NEWS2, MEWS, and SIRS were more sensitive for the diagnosis of sepsis than qSOFA (don't forget that there is no ideal tool to screen for sepsis that has both high sensitivity and specifcity).
=> NEWS2 had the greatest sensitivity and specifcity compared with MEWS, SIRS, and qSOFA.
=> qSOFA, while having a lower sensitivity for sepsis than other tools, is still useful for detecting clinical deterioration.
Identifying the causative organism in sepsis helps to optimize antimicrobial therapy, ensure that the causative pathogen is treated, support antimicrobial stewardship, and improve patient outcomes. A pathogen is identifed in approximately 60–70% of patients with sepsis, although blood cultures are positive in only approximately 10–20% of patients.
=> Given the high mortality and morbidity associated with sepsis and the importance of appropriate antimicrobial coverage, the panel issued a strong recommendation for collection of blood cultures. Blood cultures should be collected as soon as possible to avoid delay in initiating antimicrobial therapy.
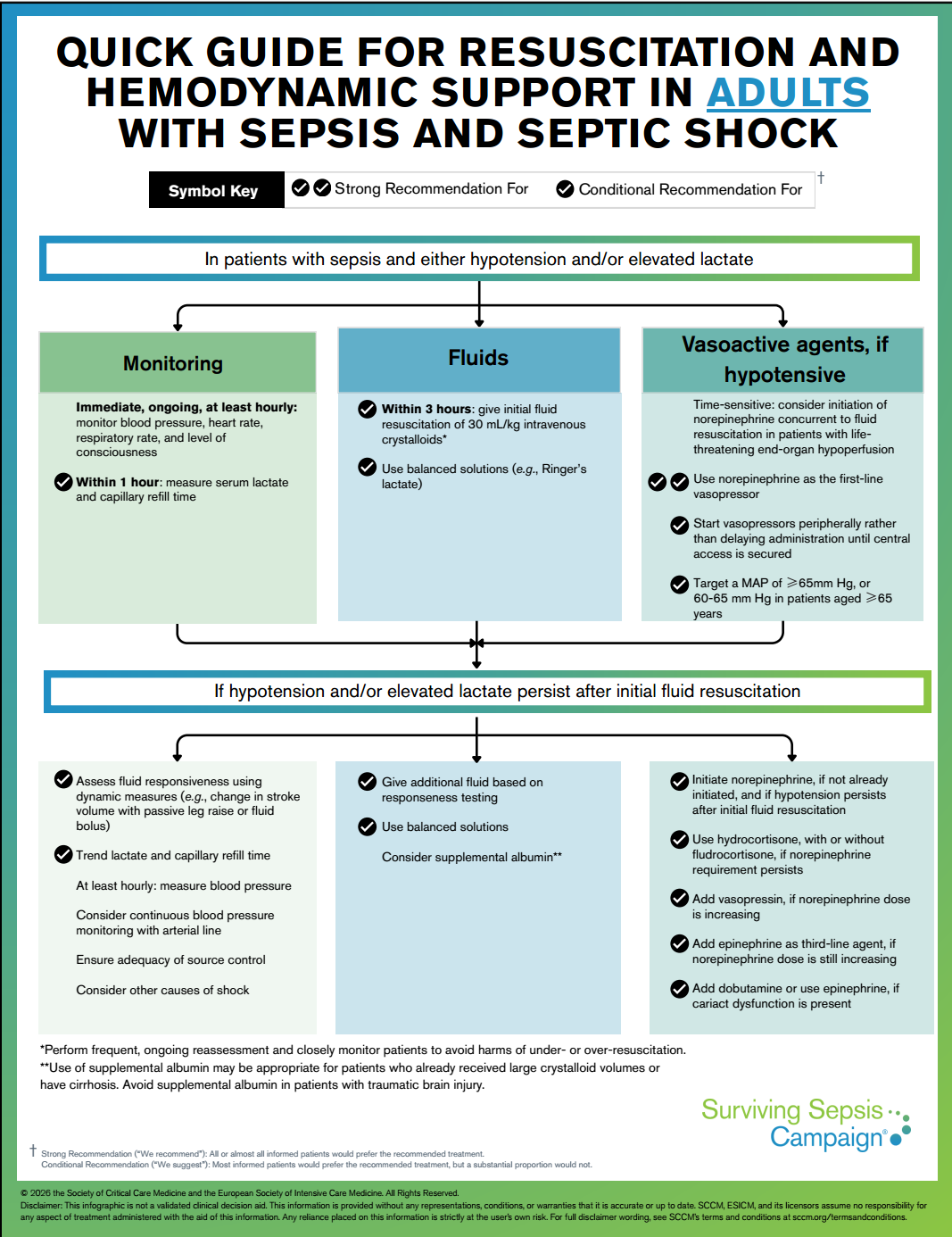
Administering at least 30 mL/kg of IV crystalloids for initial fuid resuscitation in patients with sepsis-induced hypoperfusion or septic shock.
=> The SSC panel acknowledges that fuid volume requirements vary across patients and encourages frequent reassessment to avoid under- or over-resuscitation. However, most patients with sepsis-induced hypotension and hypoperfusion beneft from greater than or equal to 30 mL/kg fuid resuscitation, and fuid-related harms generally occur with far larger volumes (e.g.,>50 mL/kg).
in progress …
Thanks to the authors.