Management of Acute Right Ventricular Failure in the Intensive Care Unit
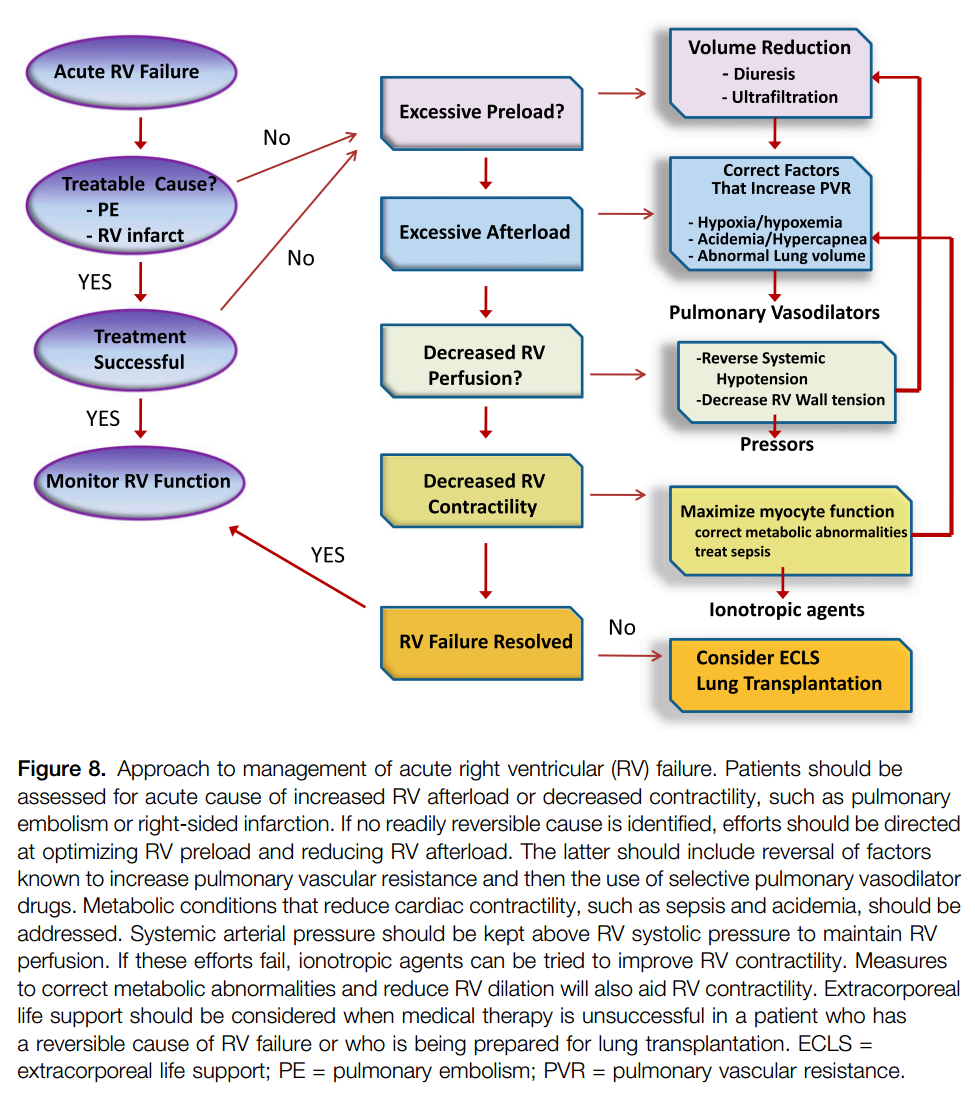
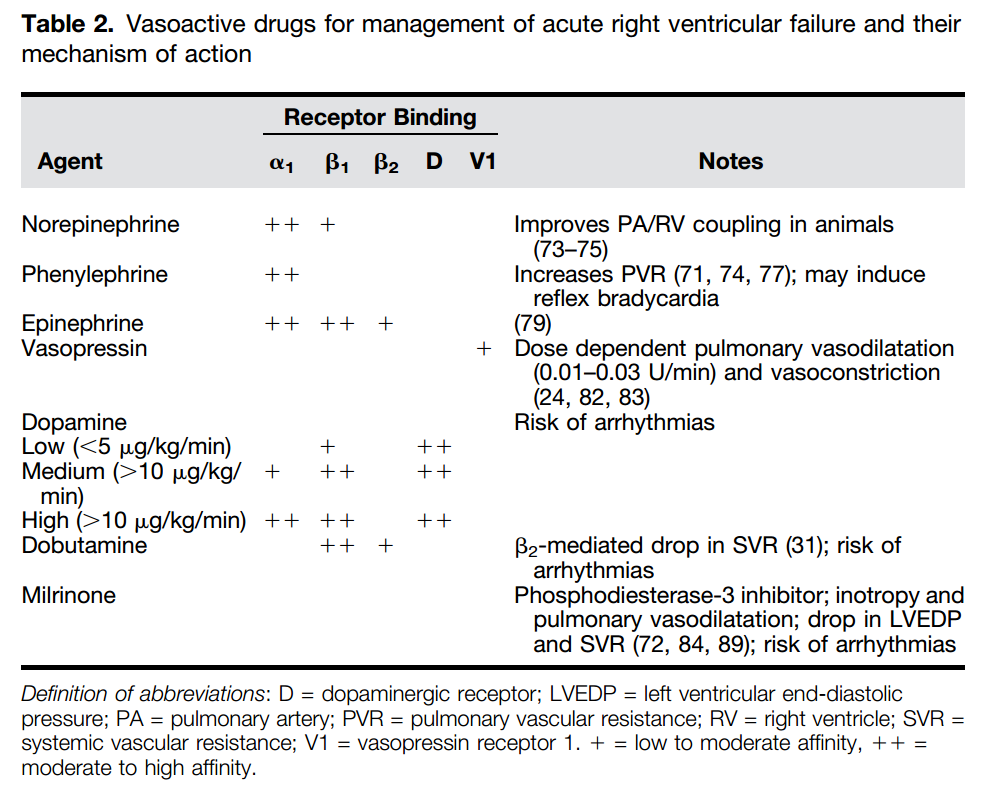
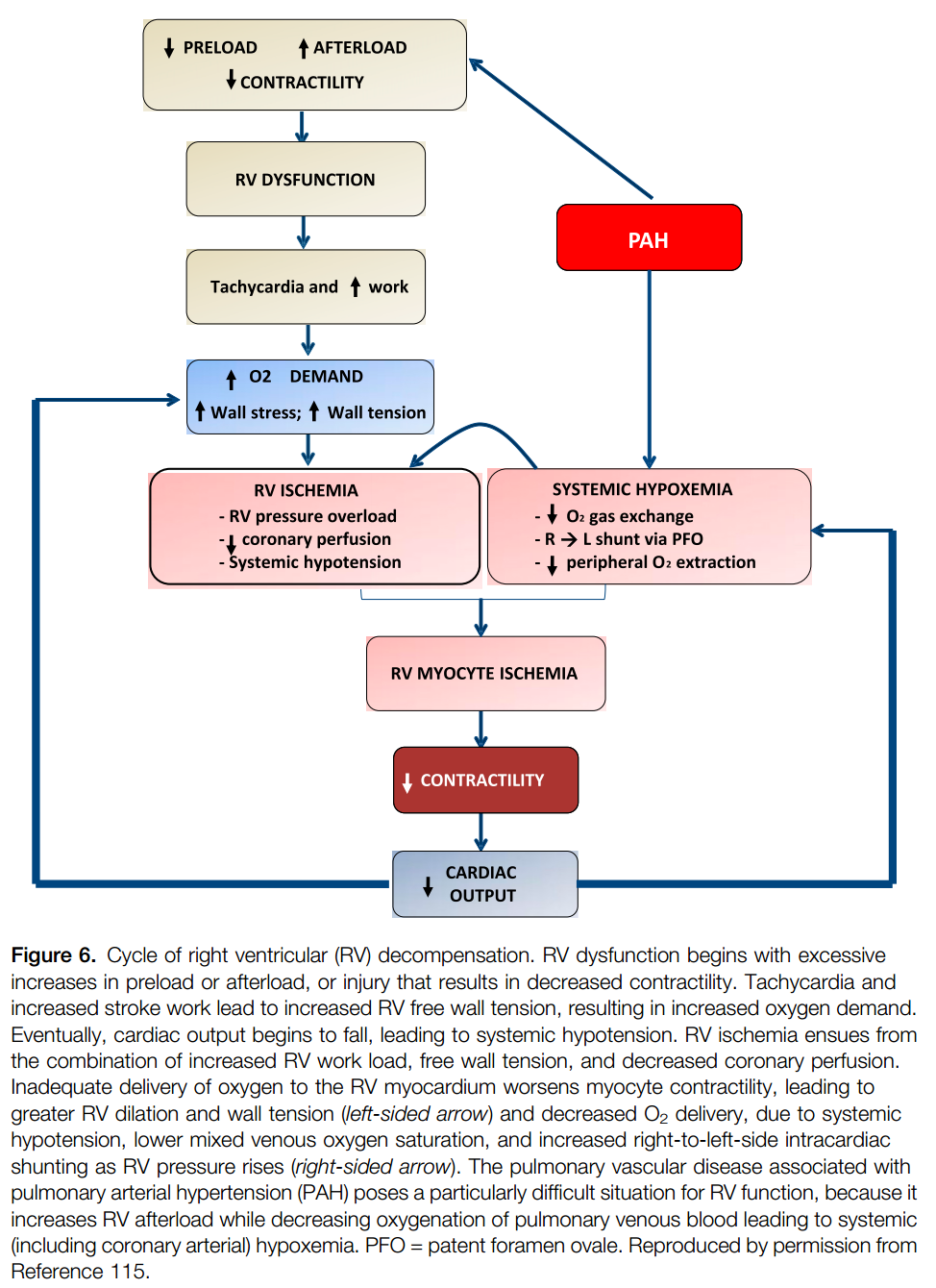
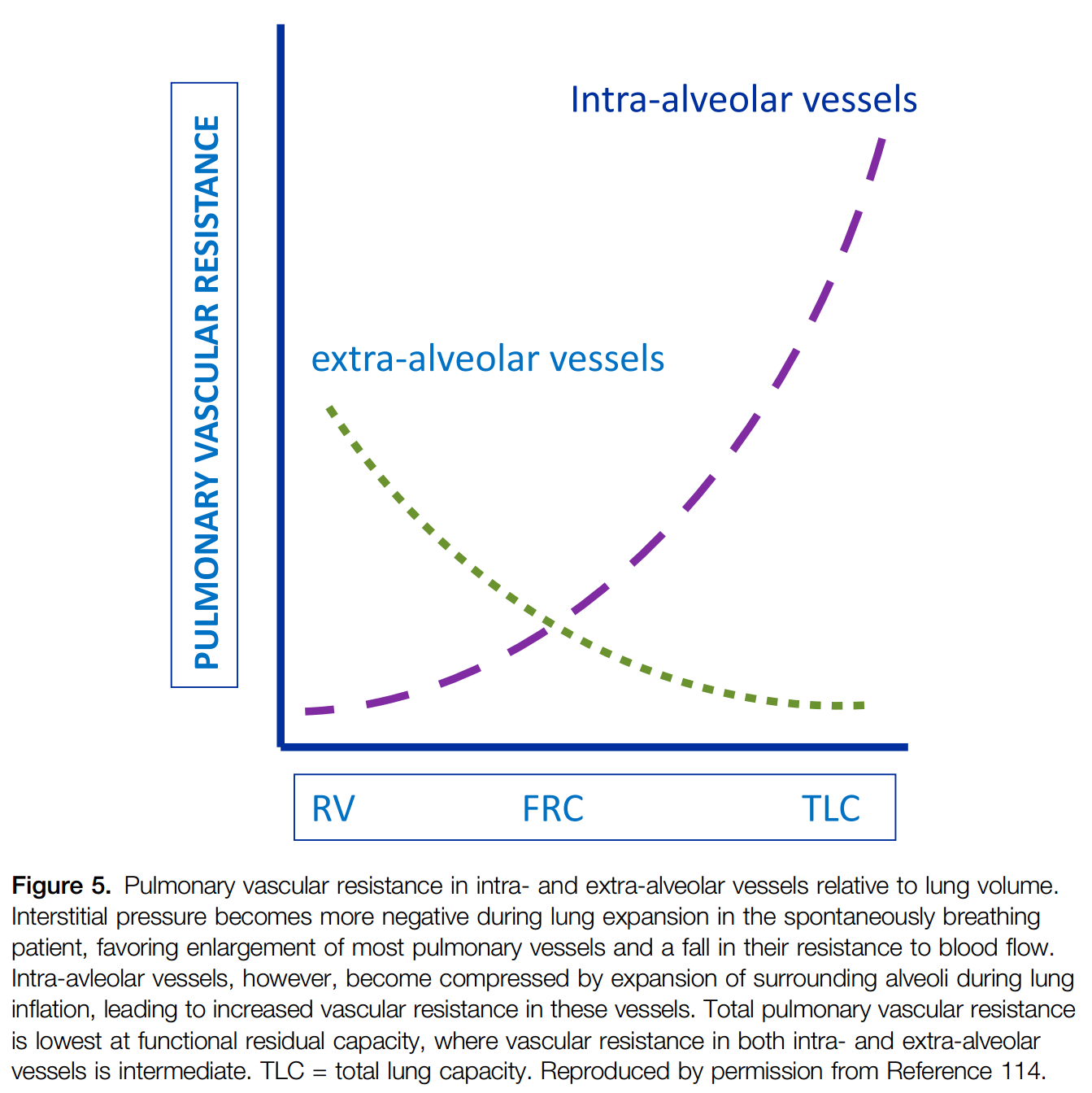
Acute RV failure is seen with increasing frequency in the intensive care unit and, when severe, can contribute to hemodynamic instability and insufficient oxygen delivery. Initial management should focus on determining the cause of RV decompensation and reversing it. When reversal is not possible, efforts should be directed toward optimizing RV preload and mitigating any factors that can increase pulmonary vascular resistance. If RV failure persists, short-acting pulmonary vasodilators should be used, preferably via inhalation in an attempt to lower RV afterload. When these efforts fail, the judicious use of vasopressors and inotropes should be considered in an attempt to improve RV perfusion and contractility.
Extracorporeal life support is effective at restoring circulatory support when other measures fail, and may be indicated in patients who are expected to recover from the cause of their RV failure, or as a bridge to surgical interventions, such as pulmonary endarterectomy or lung transplantation